
Chronic constipation rarely comes down to fiber. Explore 8 functional medicine root causes most workups miss, and what real chronic constipation treatment looks like
If you have spent years dealing with chronic constipation, you have probably already tried the obvious things. More fiber. More water. Prunes. Magnesium citrate from the drug store. Maybe a daily over-the-counter laxative that you now feel like you cannot stop using. And yet, you still feel bloated, sluggish, and stuck. You have likely been told your labs are normal, your colonoscopy looks fine, and you should just keep working on your diet. The problem is that this advice quietly assumes constipation is a single problem with a single fix, when in clinical practice it is almost always a signal that something deeper in the body is off.
This article walks through eight root causes of chronic constipation that a thorough functional medicine workup looks for, why the standard fiber-first advice misses most of them, and what a more complete approach can look like. The focus is on adults who have already tried the usual recommendations and want to understand what else might be driving their symptoms. At Integrative Wellness Centers, our care team has worked with thousands of patients since 2012 on exactly this kind of long-running, frustrating digestive issue, looking for what is actually behind the symptom rather than just managing it.
If you have been searching for answers about chronic constipation and feel like conventional approaches have not addressed the root cause, you are not alone.
Chronic constipation is not just uncomfortable, it is one of the most common gastrointestinal complaints in the country. Published prevalence data consistently estimates that around 15 percent of adults experience chronic constipation, with rates climbing to roughly 30 percent in adults over 60. Yet only a fraction of those people ever get past the surface-level advice of more fiber and more water.
Left unaddressed, persistent constipation puts a slow strain on the body. When stool sits in the colon for too long, the gut microbiome shifts, inflammation often rises, and the liver has to work harder to process recirculated waste. Many patients with long-standing constipation also report fatigue, brain fog, skin breakouts, mood changes, and stubborn weight gain. None of those are coincidences. The gut is closely tied to the immune system, the hormone system, and the nervous system, so when the bowel slows down, the rest of the body tends to feel it.
There is also a quieter cost. People with chronic constipation often quietly reshape their lives around their symptoms, avoiding meals before social events, dreading travel, and developing anxiety about food. Treating chronic constipation seriously is not just about how often you go. It is about giving your body the conditions it needs to function the way it was designed to function.
Clinically, chronic constipation is defined as a pattern of difficult, infrequent, or incomplete bowel movements that has been going on for at least three months. The Cleveland Clinic outlines the most common signs, which include fewer than three bowel movements per week, hard or lumpy stool, straining, a sense that you have not fully emptied, and needing to use manual maneuvers or pressure to pass stool.
Most people with chronic constipation recognize themselves in at least three or four of these patterns. The everyday version of chronic constipation often looks like this:
It is also worth knowing that constipation can swing back and forth with diarrhea, especially in people with irritable bowel syndrome, small intestinal bacterial overgrowth, or pelvic floor issues. If your pattern has been off for months or years, you are dealing with a chronic problem even if every individual day feels different.
The standard medical workup for chronic constipation is built around ruling out the most dangerous causes first. That is appropriate and important. Your primary care provider or gastroenterologist will usually check basic labs, rule out red flags like blood in the stool or unexplained weight loss, and, when indicated, order a colonoscopy. Once those are clear, the conversation almost always returns to fiber, hydration, exercise, and an over-the-counter laxative.
The trouble is that the in-between space, where the body is not in immediate danger but is clearly not working right, gets very little attention. Standard thyroid testing is a good example. A patient with sub-optimal thyroid function can have a TSH that sits inside the broad medical reference range while their actual thyroid hormone activity is low enough to slow the gut. That patient is told their thyroid is fine, even though their bowel is moving like it is anything but.
Fiber is the other half of the story. Harvard Health has written plainly about this: adding fiber works for some people, but in patients with more severe or complicated constipation, more fiber can actually make symptoms worse and trigger gas, bloating, and discomfort. This is especially true for people with methane-dominant SIBO, IBS-C, low motility, or pelvic floor dysfunction. Piling fiber on top of a backed-up, dehydrated, or dysmotile gut is a bit like adding more cars to a traffic jam. The road does not magically clear, it just gets fuller.
None of this is a critique of the conventional system. It is simply a recognition that ten-minute visits and population-level guidelines are not designed to find the kind of overlapping, lifestyle-related, individualized root causes that drive most long-running chronic constipation. That is exactly the gap functional medicine was built to fill.
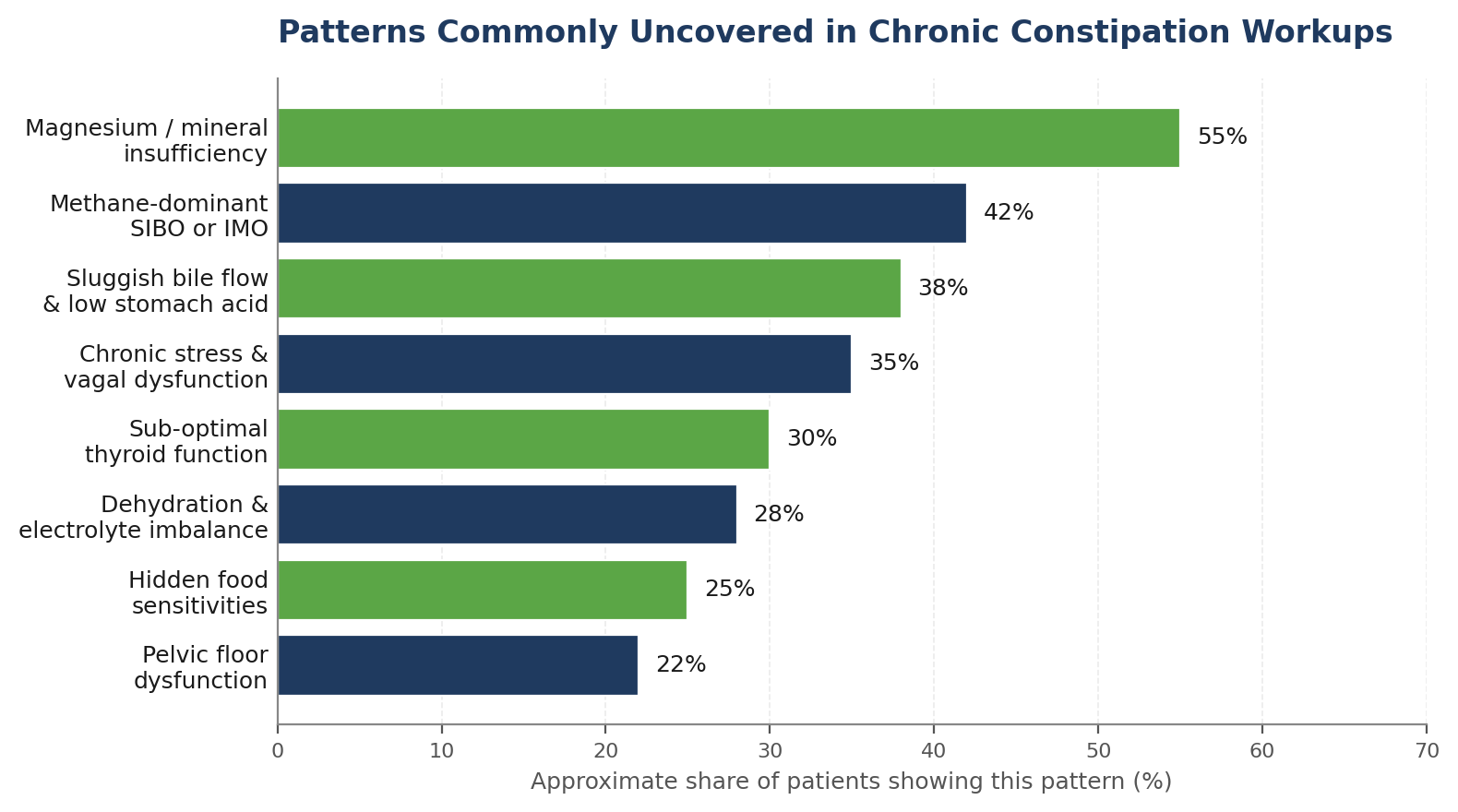
Below are eight of the most common root causes we see in functional medicine workups for chronic constipation. They are not mutually exclusive. In fact, most patients have at least two or three on this list working against them at the same time, which is part of why fiber alone rarely solves the problem.
The thyroid sets the speed of the whole body, including the gut. When thyroid hormone is low or under-converted, intestinal smooth muscle moves more slowly, stool sits longer, and water gets pulled back out, making stool harder. Research on thyroid dysfunction and gastrointestinal motility consistently shows that hypothyroidism is associated with delayed bowel transit and chronic constipation, and that these changes can be present even when standard thyroid testing looks normal.
In our experience, most patients with chronic constipation have never had a complete thyroid panel run. A complete panel goes beyond TSH to include Free T3, Free T4, Reverse T3, and thyroid antibodies. Looking at the full picture against optimal ranges, rather than the broad medical range, often reveals a thyroid that is not in immediate trouble but is clearly not supporting normal motility.
Small intestinal bacterial overgrowth has two general flavors. The hydrogen-dominant version tends to cause diarrhea. The methane-dominant version, increasingly called Intestinal Methanogen Overgrowth, or IMO, tends to cause constipation. A 2023 review published in PMC notes that methane gas directly slows intestinal transit, which is why methane positivity is strongly associated with constipation-predominant IBS and chronic functional constipation.
Patients with methane-dominant SIBO often describe bloating that gets dramatically worse with high-fiber or high-fermentable foods. They feel best on a more limited diet, get worse on the standard advice to eat more vegetables, and never fully respond to laxatives. Standard testing misses this entirely. A three-hour lactulose breath test that includes methane measurement is needed to identify it, and treatment usually involves a combined antimicrobial, dietary, and motility-support approach rather than more fiber.
Magnesium is involved in over 300 enzymatic reactions in the body, including the relaxation of smooth muscle in the intestinal wall and the regulation of fluid movement into the bowel. An NHANES analysis of nearly 9,500 US adults found that higher dietary magnesium intake was significantly associated with a lower prevalence of chronic constipation, with the highest intake quartile showing dramatically reduced odds compared with the lowest.
This is one of the most under-appreciated drivers of chronic constipation. Modern diets are low in leafy greens, nuts, and seeds, the soil is more depleted than it used to be, and stress drains magnesium out of the body quickly. Many patients turn the corner on chronic constipation just by addressing magnesium intake correctly, choosing the right form for their situation, and addressing other minerals like potassium and sodium that work alongside it. This is not a recommendation to start a supplement on your own. The right form and dose depend on your full picture.
Bile is the body’s natural laxative. When bile flow from the liver and gallbladder is sluggish, stool becomes drier, harder, and slower to move. People who have had their gallbladder removed often describe a long, complicated road of constipation alternating with urgency. People who have had years of low-fat dieting, oral contraceptive use, or chronic stress can also end up with congested bile flow even with the gallbladder intact.
Low stomach acid sits right alongside this. When stomach acid is low, food is not broken down well in the first place, the small intestine does not get the right signals to release bile and pancreatic enzymes, and motility through the entire digestive tract slows. Aging, chronic stress, long-term use of acid-suppressing medications, and certain nutrient deficiencies all push stomach acid lower than it should be. Restoring proper digestive output is often a quietly powerful piece of resolving chronic constipation.
Digestion is parasympathetic. The body literally calls it the rest and digest state. The vagus nerve is the main highway between the brain and the gut, and when it is well-toned, bowel movements happen easily, often within an hour of a meal. When the nervous system is locked in a fight or flight pattern, that signaling weakens. Blood flow shifts away from the gut, motility slows, and the urge to go fades.
Many chronically constipated patients live in a low-grade sympathetic state without realizing it. They wake up tired but wired, push through the day on caffeine, eat lunch in front of a screen, and wonder why they cannot go. Working on nervous system regulation is not soft science. It is biology. Patients who add slow morning routines, vagal exercises, paced breathing, and proper rest often see motility shift before any supplement is added.
Most patients with chronic constipation hear the advice to drink more water and assume it does not apply to them because they already drink a lot. The real issue is rarely just total volume. It is what happens to that water once it gets into the body. Without enough sodium, potassium, and magnesium, the body cannot hold onto fluid in the right places, and the colon ends up pulling water back out of stool to use elsewhere.
High-fiber advice without proper hydration support is a classic mistake. Fiber needs water to do its job. If you pile on bran, psyllium, or extra vegetables without enough water and the minerals that help retain it, you end up with bulkier, harder stool that is even more difficult to move. Hydration is not just an instruction to drink. It is a function of how well your body is using what you drink.
Food sensitivities are different from food allergies. They do not cause hives or anaphylaxis. They cause delayed, low-grade inflammation in the gut lining that can quietly slow motility, alter the microbiome, and contribute to constipation. Gluten and dairy are the two most common culprits in chronic constipation, but eggs, soy, corn, and certain food additives also show up regularly.
Patients with undiagnosed non-celiac gluten sensitivity, in particular, often live for years with constipation, bloating, and brain fog before realizing food is part of the picture. A structured elimination protocol, sometimes paired with targeted food sensitivity testing, can clarify which foods are actually contributing. The goal is not to remove foods forever, it is to identify the few that are slowing you down so the rest of your diet can do its job.
This one is often missed entirely. The pelvic floor is a group of muscles that has to coordinate properly to allow stool to pass. If those muscles are too tight, do not relax on cue, or contract at the wrong moment, stool simply cannot exit even when it has made it all the way through the colon. People with pelvic floor dysfunction often describe straining for long periods, feeling stool is right there but will not come out, or needing to use unusual positions or pressure to evacuate.
Common contributors include past childbirth, abdominal surgery, chronic core tension, a history of holding stool, and chronic anxiety. No amount of fiber or laxative will fix a mechanical coordination problem. Recognizing it and referring to qualified pelvic floor physical therapy when indicated is part of a complete plan, alongside addressing the other physiological drivers above.
The contrast between a standard workup and a functional medicine workup becomes clearer when you put them side by side. The table below shows the kind of differences our care team sees most often between the two approaches.
Functional medicine starts from a different question. Instead of asking how do we make the symptom less annoying, it asks what is actually going wrong in this body, and why. For chronic constipation, that question opens up a much wider field of testing and treatment. You can read more about this kind of work on our digestive issues page, which covers the broader category that chronic constipation falls into.
The starting point is a thorough lab workup that goes well beyond the basics. Our team uses a comprehensive functional blood panel that evaluates more than 80 biomarkers across the thyroid, immune, liver, kidney, and nutrient categories, reviewed against optimal ranges rather than just medical ranges. When the picture suggests it, we add targeted testing such as GI-MAP stool analysis, SIBO breath testing, DUTCH hormone panels, food sensitivity testing, and mold or mycotoxin testing. You can see how this kind of broad assessment works on our advanced lab testing page.
Once the testing is back, the care team builds a personalized plan that addresses what is actually showing up rather than what is most common. Two patients with chronic constipation can end up with very different plans. One might need thyroid support, mineral repletion, and food sensitivity work. Another might need antimicrobial support for methane SIBO, vagal nerve work, and bile flow support. The plan is the patient, not a template.
Chronic conditions do not unwind in a single visit. A typical care plan with our team spans four to seven months and includes scheduled follow-ups, lab rechecks at key intervals, and direct contact with the care team between visits. This is not about handing you a list and sending you off. It is about staying close to the case until the underlying drivers are addressed and the symptoms have actually shifted.
Understanding the root cause of chronic constipation starts with the right testing and a care team that takes the time to listen. Integrative Wellness Centers offers in-person care across Michigan and Zoom consultations for patients in most US states. If you are ready to stop guessing and start getting answers, you can book a consultation with our functional medicine team.
Recovery from long-standing chronic constipation is rarely a single dramatic moment. It is a series of quiet changes that add up over a few months. For many patients, the first thing that shifts is energy and bloating, often within the first few weeks of addressing thyroid, mineral, or food sensitivity drivers. Bowel patterns usually start to normalize a little later as the gut microbiome rebalances and motility returns.
A typical four to seven month care plan progresses through three rough phases. In the first phase, the focus is on calming inflammation, restoring nutrients, and removing obvious triggers. In the second phase, the focus shifts to addressing specific findings like SIBO, low thyroid function, or pelvic floor coordination. In the third phase, the work is about consolidating gains, supporting the nervous system, and giving the body the time it needs to settle into a new normal.
The body is designed to be self-healing and self-regulating when it is given the right conditions. That is not a slogan. It is what tends to happen when sleep is good, stress is manageable, nutrients are adequate, the gut is not under attack from chronic infections or food sensitivities, and the nervous system is allowed to spend more time in a parasympathetic state. Most patients with chronic constipation have not had all of those conditions at once in a long time. Giving them back, one by one, is most of what real recovery actually looks like.
Chronic constipation is rarely a fiber problem. It is usually a signal that something else is off, often a combination of sub-optimal thyroid function, methane-dominant SIBO, mineral insufficiency, sluggish bile flow, chronic stress, food sensitivities, or pelvic floor coordination. A functional medicine workup uses comprehensive testing and root-cause thinking to identify which of these drivers are at play in your specific case, which is why patients who have already maxed out fiber and laxatives often see real change once the full picture is finally assessed.
Integrative Wellness Centers works with patients in-person across Michigan and via Zoom in most US states to identify what is actually driving these symptoms. You can schedule a new patient consultation to talk through your specific history with our care team.
These are some of the questions patients ask most often when they come in with a long history of chronic constipation. The answers below are general and educational. Your specific situation may look different, which is why an individualized workup matters.
1. What does chronic constipation feel like, and how is it different from occasional constipation?
Chronic constipation feels like a persistent backed-up state that does not fully clear no matter what you eat. The clinical threshold is symptoms for at least three months, usually with fewer than three bowel movements per week, hard or pellet-like stool, straining, or a sense of incomplete emptying. Occasional constipation, by contrast, comes and goes with travel, stress, or a temporary diet change and resolves on its own within days.
2. Will chronic constipation go away on its own?
Sometimes mild, recent constipation does resolve on its own once life stress, dehydration, or a diet change passes. True chronic constipation, the kind that has gone on for months or years, almost never resolves without identifying and addressing what is driving it. The longer it has been going on, the more likely there are multiple overlapping causes.
3. Why doesn’t fiber help my chronic constipation?
Fiber helps when the root cause is genuinely low fiber intake and the rest of the system is working. For most chronic cases, the root cause is something else, such as low thyroid function, methane SIBO, magnesium insufficiency, or pelvic floor dysfunction. In those cases, more fiber can actually worsen bloating, gas, and stool quality, because the underlying mechanism has not been addressed.
4. Can chronic constipation cause weight gain, fatigue, or skin issues?
It is more accurate to say that chronic constipation and those issues often share root causes. Sub-optimal thyroid function, gut microbiome imbalance, food sensitivities, and chronic stress can all express themselves as constipation, fatigue, weight changes, and skin issues at the same time. Addressing the root causes tends to improve more than one symptom at once.
5. What causes chronic constipation in women specifically?
Women have a higher rate of chronic constipation than men for several reasons. Hormonal shifts around the menstrual cycle, pregnancy, and perimenopause influence motility. Pelvic floor dysfunction is more common after childbirth. Thyroid dysfunction is more prevalent in women. And women are statistically more likely to live with the chronic low-grade stress patterns that suppress vagal tone and slow digestion.
6. How long does it take to fix chronic constipation with a functional medicine approach?
Most care plans for chronic digestive issues run four to seven months, with meaningful improvements often appearing in the first six to twelve weeks. The exact timing depends on how many root causes are active, how long symptoms have been going on, and how consistently the plan is followed. The goal is durable change, not a quick fix that comes back the moment a supplement is stopped.
7. When should I see a doctor about chronic constipation?
Any constipation that comes with blood in the stool, unexplained weight loss, severe pain, or a sudden change in bowel habits should be evaluated promptly by a medical doctor to rule out serious causes. Outside of those red flags, if symptoms have lasted more than a few months and standard advice has not helped, it is worth working with a clinician who can investigate the underlying drivers rather than continuing to manage the symptom in isolation.
If this article resonated with what you have been going through, the next step is finding out whether functional medicine is the right fit for your situation. Integrative Wellness Centers has supported thousands of patients since 2012, both in-person across Michigan and via Zoom in most US states. You can request a new patient consultation to start the conversation with our care team.
Medical Disclaimer
This article is for informational and educational purposes only. It is not intended as medical advice and should not replace consultation with a qualified healthcare provider. Integrative Wellness Centers makes no claims to diagnose, treat, cure, or prevent any disease. Always consult your doctor before making changes to your health regimen or discontinuing any medication.

Take the online digestive evaluation to instantly discover what systems of your body are the cause of your health issues.
Online Digestive EvaluationTake the TestOnline Female Hormone EvaluationOnline Male Hormone Evaluation


